At the beginning of the pandemic, we observed that lithium carbonate had a positive effect on the recovery of severely ill patients with COVID-19. Lithium is able to inhibit the replication of several types of viruses, some of which are similar to the SARS-CoV-2 virus, increase the immune response and reduce inflammation by preventing or reducing the cytokine storm. Previously, we published an article with data from six patients with severe COVID-19 infection, where we proposed that lithium carbonate could be used as a potential treatment for COVID-19. Now, we set out to conduct a randomized clinical trial number EudraCT 2020–002008–37 to evaluate the efficacy and safety of lithium treatment in patients infected with severe SARS-CoV-2. We showed that lithium was able to reduce the number of days of hospital and intensive care unit admission as well as the risk of death, reduces inflammatory cytokine levels by preventing cytokine storms, and also reduced the long COVID syndromes. We propose that lithium carbonate can be used to reduce the severity of COVID-19.
Introduction
Since COVID-19 (coronavirus infectious respiratory disease 2019) and the responsible virus, SARS-CoV-2 (severe acute respiratory syndrome coronavirus 2), were described in December 2019, there has been no effective antiviral treatment for patients. Worldwide, this disease has affected more than 213 million people and has already killed more than 4 million (WHO, August 2021 data).
Clinical manifestations of COVID-19 range from asymptomatic infection to bilateral pneumonia, acute respiratory distress syndrome (ARDS), cytokine storm, coagulopathy, thrombosis, and other extrapulmonary syndromes (Woolhouse et al., 2012). Although this infection is characterized by respiratory symptoms, numerous studies have shown that patients infected with SARS-CoV-2 can have other organs such as the heart, kidneys, gastrointestinal tract, brain, and liver affected (Oldstone et al., 1993).
This pandemic is currently being combated by immunizing the population with different vaccines developed in many countries. However, focusing the strategy only on vaccination is showing many weaknesses: the constant appearance of new variants, the large number of people who refuse vaccines worldwide, the difficult access to the vaccine for a large part of the world population, and the percentage of people who once infected suffer a rapid deterioration of their health and end up in hospital. This scenario is indicating to us the importance of developing effective treatments for those infected with COVID-19 that will help us in the management of this disease.
Therefore, a potent antiviral agent that can be administered in the early stages of infection is urgently needed. In the absence of a specific treatment against this new virus, different drugs have been tested since the beginning of the pandemic, such as hydroxychloroquine and chloroquine, two antimalarial agents (Antia et al., 2003; Greenwood, 2014). Treatment with hydroxychloroquine was shown to be of no benefit and was associated with increased mortality in patients with COVID-19 (De Clercq and Li, 2016). Another treatment used in many patients was remdesivir (GS-5734) (Wang et al., 2020), a viral RNA polymerase inhibitor that had demonstrated in vitro antiviral activity against SARS-CoV-1 and MERS-CoV (Cunningham et al., 2020). However, this treatment showed no clinical benefit in hospitalized patients (Cascella et al., 2022; Gao et al., 2020). The same was true for the lopinavir/ritonavir combination, a treatment used for HIV prevention. Although lopinavir had demonstrated in vitro activity against SARS-CoV-2 (Hao et al., 2015; Duvall and Gallicchio, 2017), ex-post clinical trials showed that the lopinavir/ritonavir combination also had no clinical benefit in hospitalized COVID-19 patients (Hao et al., 2015; Zhao et al., 2020).
Other immune-modulating treatments have been administered in some patients, such as TNFα inhibitors that block the interaction of the cytokine with its receptors p55 or p75 (infliximab, adalimumab, certolizumab) (Ayuso, 1994; Chen et al., 2015; Cui et al., 2015; HJ et al., 2018). Some monoclonal antibodies, such as anti-IL6 (tocilizumab) or anti-Receptor IL6 (sarilumab) showed in a recent meta-analysis a slight decrease in 28-days mortality (Karampitsakos et al., 2021; Mariette et al., 2022), and more recently, sotrovimab, a SARS-CoV-2 neutralizing antibody, showed a reduction in the risk of disease progression (Gupta et al., 2021). Thus, with these types of biologic therapies, it has been concluded that these drugs should be used in specific types of patients, such as individuals with very high levels of IL-6. Finally, the recovery study concluded that, of all the therapies tested, dexamethasone 6 mg for 7–10 days was the one that showed the best results and is the currently accepted therapy in all hospitals (Horby et al., 2021; Munch et al., 2021).
The COVID-19 pandemic has highlighted the lack of effective antiviral compounds. Paxlovid (Pfizer), the first antiviral drug for COVID-19, has recently been approved. Paxlovid reduces the chance of hospitalization or death by 89% (Mahase, 2021). Molnupiravir (developed by Merck) has been shown to be highly effective in reducing infectious virus and SARS-CoV-2 viral RNA in the nasopharynx, reducing the risk of hospitalization and death by approximately 50% compared with placebo for patients with mild or moderate COVID-19 (Holman et al., 2021; Willyard, 2021). These new drugs open up the possibility for patients to be treated at home, with a combination of a capsule and a pill, but cost and access to these drugs remain serious obstacles. The continuing rise in hospitalizations and deaths following the approval of these drugs demonstrates this.
Since the beginning of the pandemic, we observed that lithium carbonate had a positive effect on the recovery of severely ill patients with COVID-19. In 2020, we published a case report article with data from six patients with severe COVID-19 infection, where we proposed that lithium carbonate could be used as a potential treatment for COVID-19 (Shorter, 2009; Rosen, 2017; Spuch et al., 2020). In that study, we showed how treatment with lithium carbonate reduced inflammation levels and rapidly increased lymphocyte levels, ostensibly improving the health of these patients compared to patients under the standard treatment used at that time.
Lithium was approved by the FDA in 1970 as a psychotropic antidepressant/mood-stabilizing drug to treat bipolar affective disorders (Won and Kim, 2017). However, lithium is also known to be involved in cellular processes such as apoptosis, proliferation, motility, gene expression, glycogen synthesis and inflammation. Recently, evidence has accumulated that lithium can also inhibit infection by DNA- and RNA-type viruses, such as HIV (human immunodeficiency virus), HSV (herpes simplex virus), infectious bronchitis virus, canine parvovirus, porcine parvovirus, pseudorabies herpesvirus, porcine reproductive and respiratory syndrome, transmissible gastroenteritis virus, vaccinia virus, feline calicivirus and, recently, coxsackievirus B3 (Skinner et al., 1980; Ziaie and Kefalides, 1989; Amsterdam et al., 1990; Gallicchio et al., 1993; Bschor, 1999; Everall et al., 2002; Harrison et al., 2007; Sui et al., 2010; Yamauchi and Helenius, 2013; Puertas et al., 2014; Ibáñez et al., 2018; Li et al., 2018; Zhao et al., 2020). Its ability to inhibit the growth of coronaviruses has also been demonstrated (Harrison et al., 2007) (Supplementary Table S1).
In the case of viral infections, Lithium exerts two types of actions; one is antiviral, and the other is its immunomodulatory effect; that is, the monovalent Li + cation exerts both neuroprotective and neurotrophic effects (Quiroz et al., 2010), which may result in immunoprotective and immunotrophic effects. The mechanism of action of lithium involves several signalling pathways such as inhibition of GSK3β (JA et al., 2004). GSK3 is an enzyme related to neuronal “pruning.” Its decrease results in increased neuronal retention. In addition, Li + ion acts competitively by binding directly to the Mg2+ binding sites of these enzymes (Hao et al., 2015). Thus, it is postulated that lithium may exert both beneficial actions to prevent poor prognosis in SARS-CoV-2 infection.
Considering its action on the immune system, lithium can mitigate the predominantly macrophagic and over-activated immune response responsible for the clinical deterioration and development of SARS. Secondly, lithium inhibits proinflammatory cytokines and will enhance the function of T lymphocytes to clear the virus from the body. In common parlance, it can change the “cytokine storm” to a “cytokine drizzle”. This led several groups to propose lithium as a possible treatment for SARS-CoV-2 (Gómez-Bernal, 2020; Murru et al., 2020; Spuch et al., 2020).
Based on these observations, we set out to conduct a clinical trial to evaluate the efficacy and safety of lithium treatment in patients infected with severe SARS-CoV-2.
Materials and Methods
Study Design
This clinical trial is a proof-of-concept study in which it is not necessary to make a formal sample size estimate. It is a prospective, longitudinal, interventional, and comparative study between a control group (n = 15), formed by patients with COVID-19 treated with standard treatment (dexamethasone 6 mg/24 h, 7–10 days) and an experimental group (n = 15), formed by patients with COVID-19 treated with standard treatment plus Lithium Carbonate (Plenur). Patients in the experimental group received 200 mg every 12 h of Lithium Carbonate, aiming for plasma levels between 0.6 and 1.2 mEq/L. In the following visits, depending on blood lithium levels, the dose could be modified, if necessary.
Patients with COVID-19 admitted to the Hospital Álvaro Cunqueiro (Vigo, Spain) were recruited. All of them were detected through the Microbiology Service by RT-PCR determinations for SARS-CoV-2. All patients who met all the inclusion criteria and none of the exclusion criteria were asked to sign the informed consent form. If obtained, 1:1 randomization was performed considering similar gender and age.
The primary outcome was assessed by measuring the number of days of hospital admission and the number of patients requiring admission to the ICU. Secondary outcomes were measured by assessing clinical and analytical parameters.
Inclusion Criteria
Patients admitted to COVID-19 older than 18 years, who did not require an ICU at the time of inclusion in the study. Detection of SARS-CoV-2 RNA in nasopharyngeal samples was performed by quantitative real-time polymerase chain reaction (RT-PCR).
Exclusion Criteria
Children under 18 years of age. Patients in whom lithium treatment was not appropriate due to their clinical condition (pregnancy and lactation; severe renal insufficiency, severe cardiovascular disease; severe dehydration or sodium depletion; hypersensitivity to lithium).
Statistical Methods
Descriptive statistical analysis was performed for all variables. Continuous variables were summarized by N, mean, standard deviation (SD), median, maximum and minimum. On the other hand, categorical variables were described by N and the percentage of each category over the total valid values. In the case of missing values, their number per variable was described. Comparisons were performed using the χ2 test or the t-test as appropriate, or other statistical tests determined in the Statistical Analysis Plan. The significance level of all statistical tests was set at 0.05.
Institutional Review Board Statement
The study was conducted in accordance with the guidelines of the Declaration of Helsinki and was approved by the Ethics Committee of the Galician Network of Research Ethics Committees (protocol code 2020/238, approval date 30/09/2020) and approval of the clinical trial by the AEMPS 06/06/2020 with number EudraCT 2020–002008–37. Written informed consent was obtained from all participants. All information collected was treated as strictly confidential, in accordance with national regulations.
Plasma Isolation
Plasma samples were obtained using BD Vacutainer™ PET EDTA Tubes centrifugation, aliquoted, and cryopreserved at −80°C until further use.
Cytokine Quantification in Plasma
Plasmas previously collected were used for the quantitative determination of cytokines (IL6, TNFα, IL2, IL10, IL12, IP10, IFNγ, sTIMP3, and IL1β by ELISA kits (Abyntek), and PD1-L1 by ELISA kit from Mybiosource according to the manufacturer’s instructions.
Markers of Inflammation and Severity of Disease
Levels of CRP and absolute lymphocyte count were recorded from the electronic medical record.
SARS-CoV-2 Viral Load Quantification
We performed nucleic acid extraction in a MicrolabStarlet IVD platform using the STARMag 96 × 4 universal Cartridge Kit (Seegene Inc., Seoul, South Korea). To detect SARS-CoV-2, we applied the Allplex™ SARS-CoV-2 Assay (Seegene Inc., Seoul, South Korea), a multiplex one-step rRT-PCR able to simultaneously detect four viral targets including the structural protein envelope (E) gene, the RNA-dependent RNA polymerase (RdRP) gene, the spike (S) gene, the nucleocapsid (N) gene, and an exogenous RNA-based internal control (IC). We targeted a conserved region in the structural protein envelope E-gene for pan-Sarbecovirus detection, RNA-dependent RNA polymerase (RdRP), and nucleocapsid (N) genes specific for SARS-CoV-2. For rRT-PCR, we employed the CFX96™ system (Bio-Rad Laboratories, Hercules, CA, United States). We analysed the results using Seegene Viewer-specific SARS-CoV-2 software (Seegene Inc., Seoul, South Korea). To establish a linear regression curve and obtain the concentration in copies/ml (inversely related to the cycle threshold value), the EDX SARS-CoV-2 Standard (Exact Diagnostics, TX, United States) containing 200,000 copies/mL of synthetic RNA transcripts from five gene targets (E, N, ORF1ab, RdRP and S Genes of SARS-CoV-2) was used.
IgG SARS-CoV-2 Quantification
For serological evaluation of patients, we used two high throughput chemiluminescent immunoassay (CLIA) assays. First, LIAISONTM SARS-CoV-2 S1/S2 IgG (DiaSorin IgG; DiaSorin, Italy), that allows a semi-quantitative detection of IgG antibodies against to the S1 and S2 subunits of the Spike protein and second, ElecsysTM Anti-SARS-CoV-2 S (Roche T; Roche, United States), which allows the quantitative detection of total antibodies against the Spike protein.
Results
A total of 30 patients (13 females and 17 males) were included in the study. Details of the characteristics of the patients in this study are presented in Table 1. The mean ± SD of age was 59.87 ± 18.28 (range 34–86) for the control group and 57.33 ± 16.29 (range 28–84) for the experimental group. The most common medical conditions were hypertension (30%), dyslipidaemia (20%), and obesity (16%). None of the patients in the lithium group had adverse effects associated with lithium carbonate medication (Supplementary Table S2).
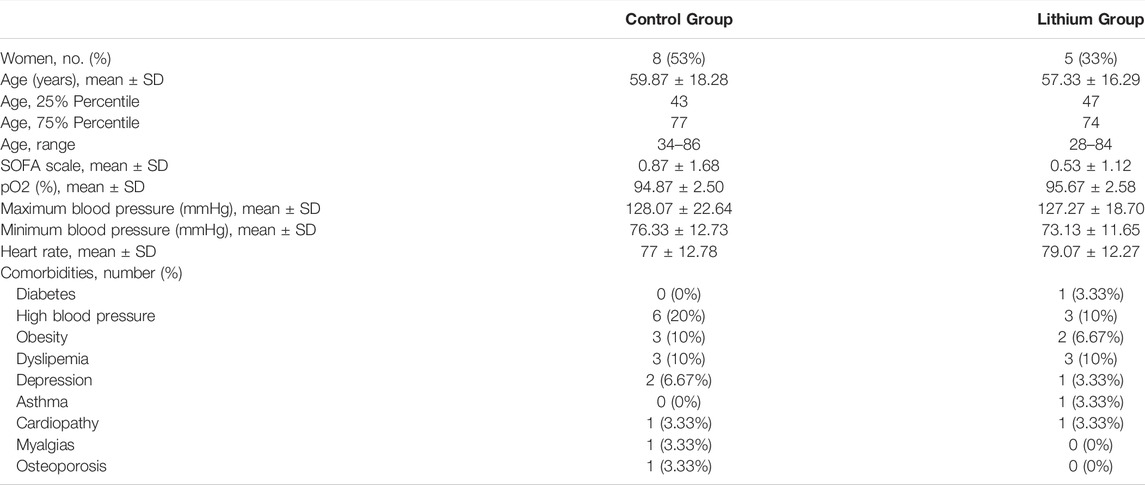 TABLE 1. Characterization of the study group.
TABLE 1. Characterization of the study group.
Lithium treatment reduced hospital days; while the control group had a mean of 12.43 days (12.43 ± 12.09), the lithium group had a mean of 6.47 days (6.47 ± 3.60) (Figure 1). The difference is not statistically significant (p = 0.17) but shows a clear trend in the reduction of hospital admission days. None of the patients who received lithium required admission to the ICU, and none of them died. In contrast, in the control group, two patients were admitted to the ICU and one patient died (Figure 1).
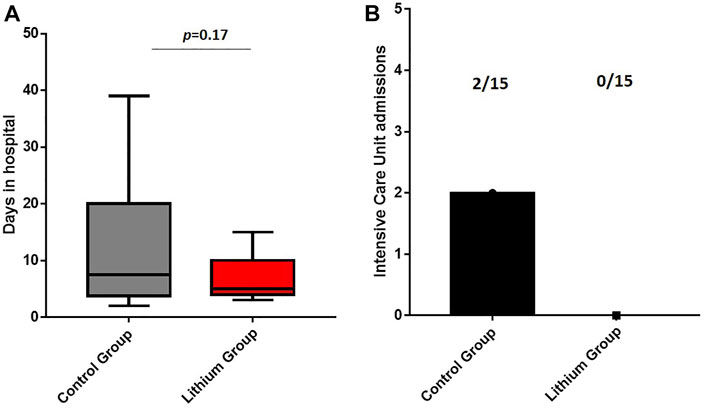 FIGURE 1. (A) Days of hospital admission. The lithium treatment group has a lower number of days of hospital admission. (B) Intensive Care Unit admissions. The control group had two intensive care unit admissions while the lithium group had no intensive care unit admissions.
FIGURE 1. (A) Days of hospital admission. The lithium treatment group has a lower number of days of hospital admission. (B) Intensive Care Unit admissions. The control group had two intensive care unit admissions while the lithium group had no intensive care unit admissions.
SARS-CoV-2 infection is characterized by marked lymphopenia, and since one of the properties of lithium is that it works as a good Immunomodulator, we investigated how it regulates blood lymphocyte levels. When we evaluated the levels of both groups during hospital admission, we clearly observed that lithium treatment significantly increased blood lymphocyte levels (Figure 2), although both groups at discharge ended up with normal blood lymphocyte levels, the lithium-treated patients recovered normal levels earlier. Patients in the control group remained 9.79 ± 11.14 days in lymphopenia, while patients on lithium treatment were only 3.87 ± 2.53 days in lymphopenia (Figure 2). With such a clear improvement in lymphocyte numbers, we decided to investigate whether lithium was able to modulate the amount of anti-SARS-CoV-2 antibodies generated after infection. We performed quantification by two different methods, the Liaison and the Roche methodology. With both methods we obtained similar results, and in both cases, there were no differences between the control group and the lithium group (Supplementary Figure S1).
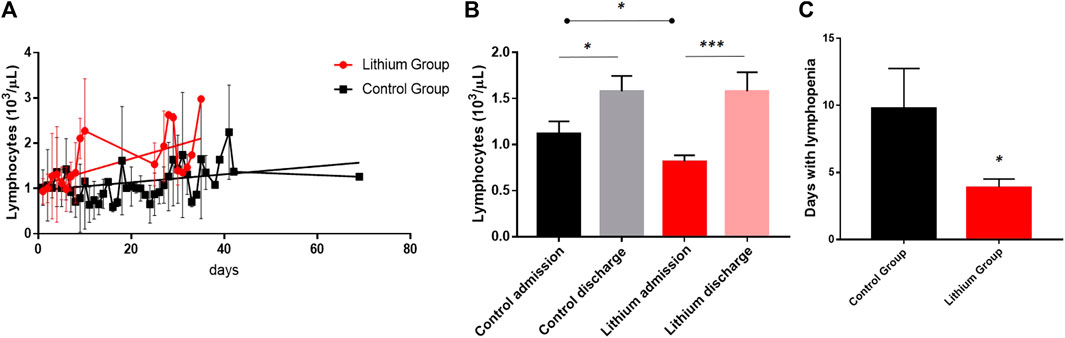 FIGURE 2. COVID-19 is characterized by very strong lymphopenia, and lithium is a modulator of the immune system. (A) In this graph we represent the mean values of lymphocytes in the two groups of the clinical trial, in red those treated with lithium and in black the control group. The lithium group recovered normal lymphocyte levels earlier than the control group. The lines show liner regression analysis, where a clear different pattern among groups is observed (p < 0.05) with different slopes for lithium group (red line, R2 = 0.3379) and control group (black line, R2 = 0.1711). (B) Although both groups recover from lymphopenia, the lithium group recovers significantly sooner by staying fewer days in lymphopenia. (C) The lithium treatment group remained significantly less days in lymphopenia than the control group (p < 0.05).
FIGURE 2. COVID-19 is characterized by very strong lymphopenia, and lithium is a modulator of the immune system. (A) In this graph we represent the mean values of lymphocytes in the two groups of the clinical trial, in red those treated with lithium and in black the control group. The lithium group recovered normal lymphocyte levels earlier than the control group. The lines show liner regression analysis, where a clear different pattern among groups is observed (p < 0.05) with different slopes for lithium group (red line, R2 = 0.3379) and control group (black line, R2 = 0.1711). (B) Although both groups recover from lymphopenia, the lithium group recovers significantly sooner by staying fewer days in lymphopenia. (C) The lithium treatment group remained significantly less days in lymphopenia than the control group (p < 0.05).
Next, we assessed the overall levels of inflammation. One of the characteristics of COVID-19 is the induction of an elevation of inflammatory parameters, strongly associated with disease severity (Tan C. et al., 2020; Tan et al., 2020 L.). In our study, we observed a favorable response of lithium treatment on inflammation, evidenced by a significant decrease in IL-6 levels (control group 792.1 ± 1128 vs. lithium group 77.83 ± 95.55, p < 0.05), TNFα (control group 952.6 ± 337.4 vs. lithium group 444 ± 59.1, p < 0.01) and IL-10 (control group 353.8 ± 68.21 vs. lithium group 206.2 ± 36.6, p < 0.05). In addition, clinical parameters on neutrophil-lymphocyte ratio (NLR) and C-reactive protein (CRP) levels, which are commonly used to detect general inflammation, were evaluated. In both cases, lithium treatment reduced the levels, not significantly but with a trend, with the NLR going from 116 ± 53.94 in the control group to 40.06 ± 6.544 in the lithium-treated group (p = 0.12). Something similar occurred with CRP levels, going from 1323 ± 491.4 in the control group to 549.7 ± 100.9 in the lithium-treated group (p = 0.15) (Figure 3).
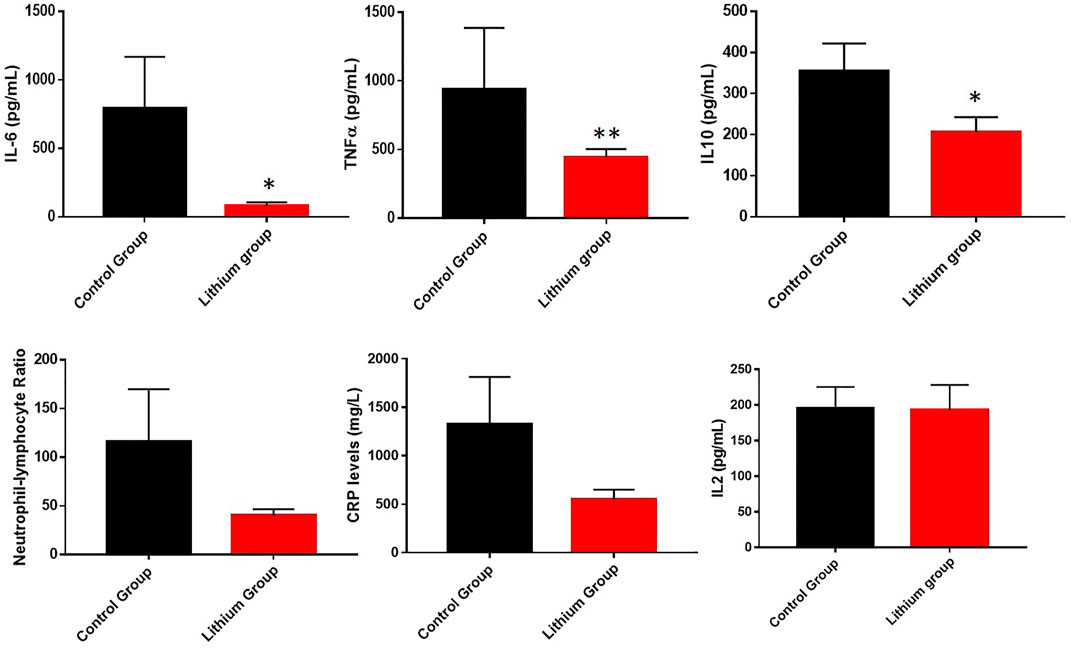 FIGURE 3. Representation of different parameters involved in general inflammation. We showed a reduction of general inflammation in the group of patients treated with lithium. The graphs represent the area under the curve of cytokine levels measured during the study. *p < 0.05 and **p < 0.01. Upper graphs represented the changes of IL-6, TNFα and IL-10 between control group and lithium group. The graphs below showed the area under the curve of the C-reactive protein graphs and neutrophil – lymphocyte ratio of all patients, control group and lithium group. We observed a tendency in the reduction of CRP levels and alower index of general inflammation without significance differences (p = 0.12 for NLR and p = 0.15 for CRP levels).
FIGURE 3. Representation of different parameters involved in general inflammation. We showed a reduction of general inflammation in the group of patients treated with lithium. The graphs represent the area under the curve of cytokine levels measured during the study. *p < 0.05 and **p < 0.01. Upper graphs represented the changes of IL-6, TNFα and IL-10 between control group and lithium group. The graphs below showed the area under the curve of the C-reactive protein graphs and neutrophil – lymphocyte ratio of all patients, control group and lithium group. We observed a tendency in the reduction of CRP levels and alower index of general inflammation without significance differences (p = 0.12 for NLR and p = 0.15 for CRP levels).
We also investigated in COVID-19 patients whose condition required ICU admission with severe acute inflammation whether lithium treatment was able to reduce cytokines involved in this level of inflammation. Indeed, lithium treatment was able to reduce the levels of most of the quantified cytokines (PD1-L1, IP10, IL-12, IL1b, IFNγ, and sTIMP3) (Figure 4). All decreased significantly, except IFNγ and sTIMP3, which showed a clear trend of decreasing levels, but the differences were not statistically significant. For IFNγ we went from 958 ± 277.6 in the control group to 374.2 ± 221.7 in the lithium-treated group (p = 0.10), for sTIMP3 we went from 1535 ± 296.3 in the control group to 1005 ± 255 in the lithium-treated group (p = 0.10).
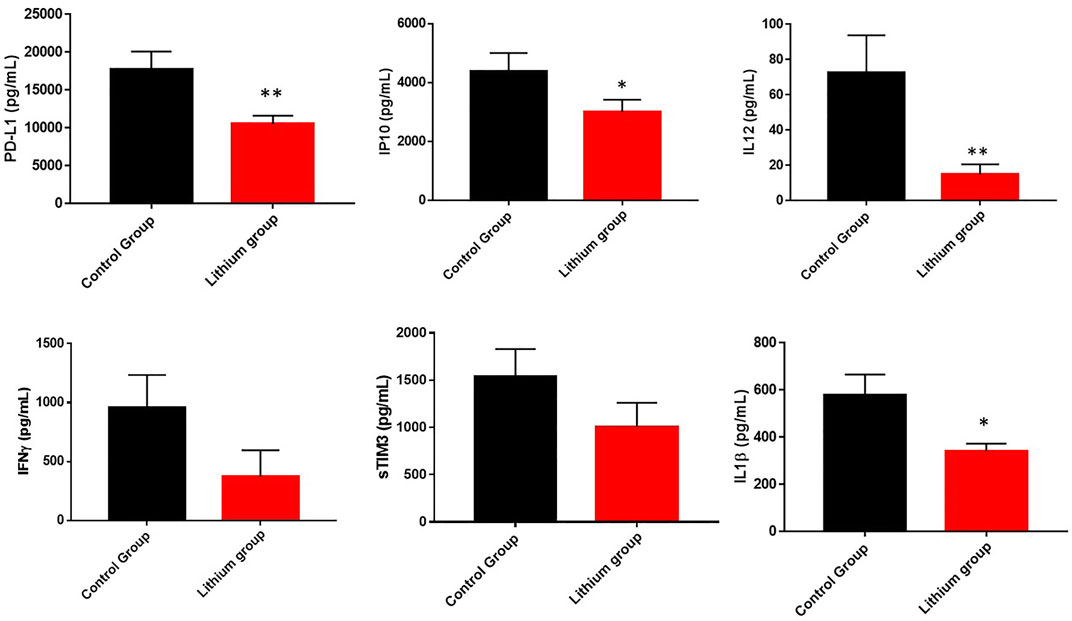 FIGURE 4. Representation of cytokine levels involved in acute inflammation (sTIM3, PD-L1, IP10, IL12, IFNγ and IL1β). These graphs showed the reduction of acute inflammation in the group of patients treated with lithium. The graphs represent the area under the curve of cytokine levels measured during the study. *p < 0.05 and **p < 0.01. In the case of IFNγ and sTIM3, there is a clear trend in the reduction of its levels in the group treated with lithium, although it is not significant (p = 0.10).
FIGURE 4. Representation of cytokine levels involved in acute inflammation (sTIM3, PD-L1, IP10, IL12, IFNγ and IL1β). These graphs showed the reduction of acute inflammation in the group of patients treated with lithium. The graphs represent the area under the curve of cytokine levels measured during the study. *p < 0.05 and **p < 0.01. In the case of IFNγ and sTIM3, there is a clear trend in the reduction of its levels in the group treated with lithium, although it is not significant (p = 0.10).
We chose to analyze the data on acute inflammatory cytokine levels temporally rather than by area under the curve during hospital admission. Temporally at admission, on day 3 (which is when the lithium treatment group generally had adequate pharmacological levels of lithium in the blood), and finally on the day of hospital discharge. On the day of hospital admission and acceptance to participate in the clinical trial, all patients had elevated inflammatory cytokines. However, on the third day, while the control group maintained elevated levels or worsened, the lithium treatment group improved significantly (Figure 5). This is important because it means that lithium may be reducing one of the main risk factors for poor patient outcomes.
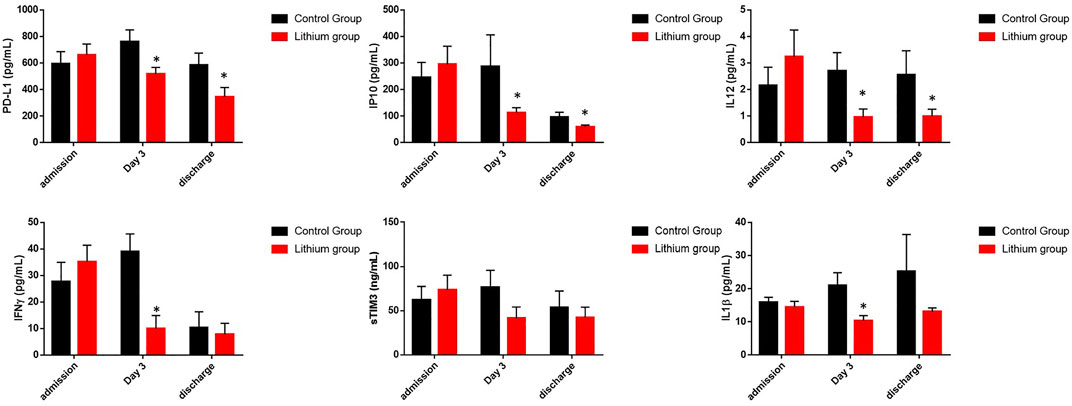 FIGURE 5. Representation of cytokine levels involved in acute inflammation measured during admission, after 3 days with treatment and during discharge. The graphs represent the area under the curve of cytokine levels measured during the study. *p < 0.05 and **p < 0.01. It can be seen how lithium treatment reduces the levels of acute inflammation after 3 days of treatment compared to the control group.
FIGURE 5. Representation of cytokine levels involved in acute inflammation measured during admission, after 3 days with treatment and during discharge. The graphs represent the area under the curve of cytokine levels measured during the study. *p < 0.05 and **p < 0.01. It can be seen how lithium treatment reduces the levels of acute inflammation after 3 days of treatment compared to the control group.
In addition, two clinical aspects that help predict whether the SARS-CoV-2 infected patient will have severe problems during admission are ferritin and D-dimer levels. We know that increased serum ferritin and D-dimer during admission predicts mortality of COVID-19 patients in the intensive care unit. In our study we observed how lithium treatment significantly reduced ferritin and D-dimer levels (Figure 6). During hospital admission both groups started from similar levels of ferritin (control group: 561.1 ± 615.20 ng/ml and lithium group: 605.5 ± 546.24 ng/ml, p < 0.05) and D-dimer (control group: 3,260.22 ± 7,346.82 and lithium group: 460.55 ± 185.46 ng/ml, p < 0.05). However, while the control group maintained elevated levels of both proteins, the lithium-treated group strongly reduced their blood levels (Figure 6).
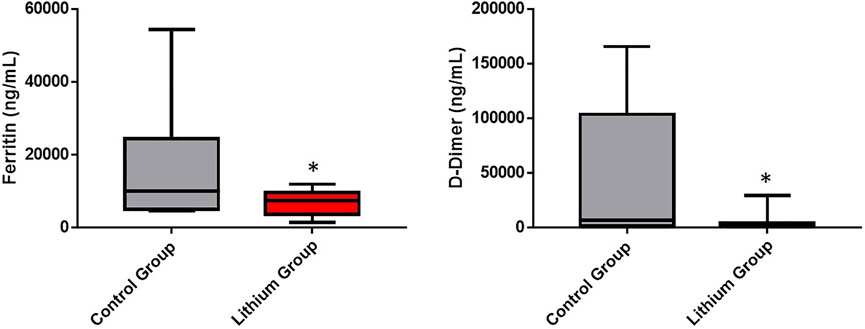 FIGURE 6. Reduction of ferritin and D-dimer levels in patients treated with lithium. The area under the curve of the ferritin and D-dimer levels of patients, control group and lithium group is quantified. Ferritin is an index that indicates the accumulation of iron and is associated with the inflammatory activity of macrophages. Lithium reduces significantly the levels of ferritin (p < 0.05). COVID-19 is usually complicated by coagulopathy. D-dimer is a maker of thrombin generation and fibrinolysis and this constitutes a relevant prognostic index of mortality from the infection. The D-dimer value is associated with the severity of patients with COVID-19. Lithium reduces significantly D-dimer levels and the risk of coagulopathy and mortality (p < 0.05).
FIGURE 6. Reduction of ferritin and D-dimer levels in patients treated with lithium. The area under the curve of the ferritin and D-dimer levels of patients, control group and lithium group is quantified. Ferritin is an index that indicates the accumulation of iron and is associated with the inflammatory activity of macrophages. Lithium reduces significantly the levels of ferritin (p < 0.05). COVID-19 is usually complicated by coagulopathy. D-dimer is a maker of thrombin generation and fibrinolysis and this constitutes a relevant prognostic index of mortality from the infection. The D-dimer value is associated with the severity of patients with COVID-19. Lithium reduces significantly D-dimer levels and the risk of coagulopathy and mortality (p < 0.05).
Since lithium has shown antiviral properties against various types of viruses, we set out to investigate whether patients on lithium treatment reduced viral load levels with respect to the control. We quantified the viral load by means of nasopharyngeal samples on the day of hospital admission and the day of hospital discharge. In this case, we found no differences between the two groups (Supplementary Figure S2).
Discussion
COVID-19 is an infection caused by the SARS-CoV-2 virus to which the immune system reacts in two phases. The first is the activation of the innate immune response, during which innate immune cells secrete interferons and cytokines to elicit the recruitment of macrophages, monocytes, and neutrophils that act as the first line of defence (Andrews et al., 2010). While this phase is developing, the second line of defence is activated, which is the adaptive immune response, activating T lymphocytes that stimulate B lymphocytes to produce specific antibodies against the virus.
One of the pathophysiological problems of COVID-19 is that it produces a maladaptive or hyper-reactive immune response, in which innate cell lineages (macrophages and neutrophils) are greatly increased, and lymphocytes greatly reduced (lymphopenia). This is associated with increased disease severity and worse prognosis, ultimately leading to intensive interventions with a high risk of intubation and mortality (Lucas et al., 2020; Qin et al., 2020).
Lithium is a drug that is part of a class of drugs called antimanic agents. It is used in the form of lithium carbonate as a mood stabilizer in people with bipolar disorder, and in Spain, it is marketed under the brand name Plenur. Lithium is used to treat and prevent episodes of mania (a frenzied and abnormally excited mood with grandiose and/or irritable behavior) in people with bipolar disorder (a disease that causes episodes of depression, suicide, mania, and other abnormal moods), and is also sometimes used in the treatment of resistant depression, schizophrenia, impulse control disorders or agitation in people with intellectual disability. It is the most effective drug in reducing suicide attempts and completed suicides (Won and Kim, 2017).
The mechanism of action of lithium is increasingly well known. It is now known that lithium exerts its action on the nervous system, specifically on brain cell retention, inhibiting glycogen synthase kinase 3β (GSK3 β) and improving conduction. As a result, neurotrophic factors, neurotransmitters, oxidative metabolism, apoptosis, and second messenger systems are modulated (Castillo-Quan et al., 2016). In simple terms, this translates into a reduction in brain aging over time. Because of these broad benefits in the CNS, lithium has also been described to have poorly understood functions in other tissues. For example, the positive effects of lithium use on various components of human blood; including, but not limited to, hematopoietic stem cells, neutrophil count, granulocyte count, thrombocyte count, dendritic cell count, and monocyte count, and on the functioning of the immune system itself through the regulation of B and T lymphocytes (Gallicchio and Chen, 1981; Barr and Galbraith, 1983; Duvall and Gallicchio, 2017). Another study shows that lithium can inhibit NF κβ nuclear translocation in macrophages and modulate the inflammatory profile after Rift Valley fever virus infection (Makola et al., 2021). Evidence was found that lithium was able to regulate both B and T lymphocytes. Interestingly, in a study on patients with thyroid hormonal imbalances, lithium was shown to be able to increase the activity of B lymphocytes and reduce the ratio of circulating suppressor T cells to cytotoxic T cells (Kibirige et al., 2013). In another recent work, lithium showed an antiapoptotic effect on T lymphocytes in patients with bipolar disorder (Pietruczuk et al., 2018).
Early in the pandemic, we began to observe that the immune system response was one of the causes of severe symptoms in COVID-19. Based on these known actions of lithium on the immune system, we conducted an observational study of six patients with bipolar disorder already taking lithium admitted to the ICU. We observed a strong improvement, especially in their inflammatory parameters (Spuch et al., 2020), a less aggressive reactivity and a more adapted response. Other comments in different publications raised the same hypothesis on the use of lithium to reduce severe symptoms caused by COVID-19 (Gómez-Bernal, 2020; Rudd, 2020; Khosravi, 2021). Based on these preliminary data, we decided to perform a randomized clinical trial with 30 patients with severe COVID-19 (EudraCT number 2020–002008–37) with two arms, a control arm with the usual treatment, in this case corticosteroid treatment, and the treatment arm with lithium added to the usual treatment. After the clinical trial, we observed that lithium treatment reduced the number of days of hospitalization, showing a clear trend. It reduced ICU (intensive care unit) admissions and death. In the control group, two patients were admitted to the ICU and one of them died, while in the lithium treatment arm, none were admitted to the ICU.
Increasing evidence points to an association between immune response and disease progression in COVID-19, in which unknown abnormalities in immune cells appear to be responsible for the uncontrolled elevation of inflammatory markers and subsequent cytokine storm, leading to disease severity and fatal outcome (Lucas et al., 2020). Therefore, finding a treatment that modulates the immune system would be key to reducing severe disease symptoms and thereby reducing ICU admission and risk of death. A treatment that is ubiquitous, inexpensive and effective would be even more valuable. COVID-19 causes a sharp drop in lymphocyte levels, which persists for many days during the disease. Several studies have found a correlation between lymphopenia and disease severity, a condition defined by abnormally low lymphocyte counts (Tan L. et al., 2020; Fathi and Rezaei, 2020; Tavakolpour et al., 2020). In our clinical trial, lithium increases lymphocyte levels much more rapidly, and lithium patients remain lymphogenic for fewer days than controls. A recent study shows that SARS-CoV-2 mainly affects lymphocytes and not innate cells (Ekşioğlu-Demiralp et al., 2021), resulting in a dysregulation of the system between the adaptive and innate immune systems. Our data show that lithium is a good treatment to rapidly increase lymphocyte levels and prevent the severity of infection.
Inflammation is a key feature of SARS-CoV-2 infection. When patients have an excessive inflammatory response, this can lead to unfavorable processes and even death. Although many infected patients are asymptomatic or have only mild or moderate symptoms, a small minority of patients develop the severe or life-threatening disease (Wong, 2020). This is because the very effects of the exacerbated immune response are more destructive than those of the infection itself, causing the so-called cytokine storm, which results in massive and irreversible damage to many organs such as the lung (Costela-Ruiz et al., 2020). When we analyzed the general parameters of inflammation in our patients, we observed elevated levels of TNF-α, IL-6, IL-10, neutrophil-lymphocyte ratio and C-reactive protein (CRP) levels. When we treated them with lithium, we observed that all general inflammation parameters were reduced. These elevated parameters, as well as lymphopenia, are a risk factor for COVID-19 morbidity and mortality, implying that lithium treatment would reduce these parameters leading to a decreased risk of disease severity.
In addition to general inflammation parameters related to cytokine storm, we decided to investigate how lithium affects different molecules related to acute inflammation and the regulation of the immune system itself, such as sTIM3 (soluble T-cell immunoglobulin mucin domain), PD-L1, IP10, IL12, IFNγ and IL1 β. Immune checkpoint molecules, such as PD-L1, sTIM3-3 and IFNγ, play an important role in regulating the host immune response and, for unknown reasons, are down-regulated in COVID-19 (Sabbatino et al., 2021; Ueland et al., 2021). IP-10, also known as CXCL10, is a proinflammatory cytokine secreted by immune cells. Together with IL12 and IL1 β it is associated with defence against various infections being highly elevated in patients with COVID-19 (Hashimoto et al., 2021; Kesmez Can et al., 2021). When we treated patients with lithium, we observed that PD-L1, IP10, IL12 and IL1 β levels were significantly reduced. In the case of IFNγ and sTIM3 values, although they are reduced with lithium treatment, it is not statistically significant. These data are evident when we calculate the levels of these proteins on the day of hospital admission, on the third day, which is when they already have lithium treatment at pharmacological doses, and on the day of hospital discharge. It was observed that on the third day all the levels of these cytokines and immune regulators were reduced, remaining constant until hospital discharge. Thus, it can be deduced that, although we do not know the mechanisms of lithium regulation on this part of the immune system, it does indicate that lithium is modulating the checkpoint mechanisms of the immune system, as well as regulating the mechanism of T lymphocyte suppression.
In addition, ferritin and D-dimer levels (two very important clinical parameters implicated in the severity of COVID-19 and in the cause of severe problems after discharge – “long COVID”-) improve in patients with lithium treatment. Ferritin is a protein related to the acute phase of immune system activation and a parameter of macrophage activity. As a hallmark of hyperferritinemic syndromes, elevated circulating ferritin is found in four critical diseases: macrophage activation syndrome (MAS), adult-onset Still’s disease (AOSD), catastrophic antiphospholipid syndrome (CAPS), and septic shock. Excessive elevation of ferritin was associated early in the pandemic with severity and high mortality risk in COVID-19 patients (Kaushal et al., 2021). D-dimer level is one of the common measures used in patients to detect thrombosis in patients with coagulopathy problems. D-dimer levels are known to be elevated in the early stages of infection and high levels are associated with poor prognosis (Rostami and Mansouritorghabeh, 2020; Terpos et al., 2020).
On the other hand, one of the most promising actions of lithium is the evidence of its action on multiple viral infections. There is evidence that lithium can inhibit the replication of several viruses, some similar and belonging to the coronavirus family (Skinner et al., 1980; Hao et al., 2015; Zhou et al., 2015). One of the objectives of this clinical trial was to determine whether lithium treatment was able to reduce viral load within a few days. However, due to methodological problems arising from clinical care due to the pandemic, it was only possible to determine the viral load on the day of admission and the day of hospital discharge. At these times there were no differences between the control and lithium treatment groups. The incubation period for COVID-19 is thought to be between 2 and 14 days after exposure, with most cases presenting symptoms approximately 4–5 days after exposure (Lauer et al., 2020), which is one of the limitations of the study, since the changes that might occur in viral load should occur during these first 2 weeks of treatment.
Another factor we wanted to determine was whether lithium treatment was able to improve the response to anti-SARS-CoV-2 antibody generation after hospital discharge (1 month after the start of the clinical trial). We performed it with two different methodologies since they were new techniques that were being introduced in hospital laboratories. We detected no differences between the two groups, indicating that survivors of infection develop optimal antibody levels.
Finally, one data that reaffirms the improvement of lithium-treated patients is that when we examined patients 1 month after hospital discharge and long-term neurological effects were recorded, 40% of lithium-treated patients were observed to have symptoms, while 73% of the control group had some neurological symptoms (Table 2). These data deserve to be investigated with a large number of patients since the reduction of neuropsychiatric symptoms of “long COVID-19” would mean a substantial improvement in the health status of the recovered patients.
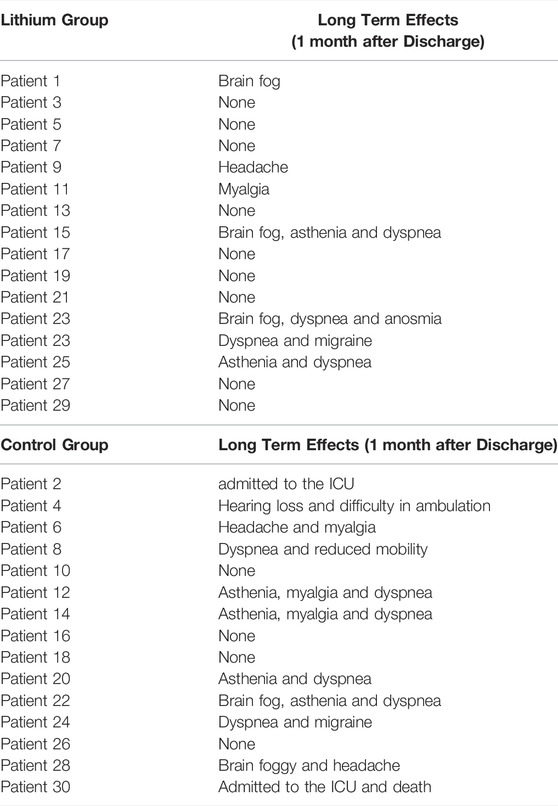 TABLE 2. Neurological long-term effects 1 month after discharge.
TABLE 2. Neurological long-term effects 1 month after discharge.
Conclusion
This randomized clinical trial demonstrates that lithium carbonate treatment is safe and effective in curbing the severity caused by SARS-CoV-2 infection. SARS-CoV-2 infection induces exaggerated inflammation driven by components of innate immunity. We demonstrated that lithium was able to reduce the number of days of hospital and ICU admission as well as the risk of death. Lithium, through its immunomodulatory action, reduces inflammatory cytokine levels by preventing cytokine storms, thus reducing the severity of the infection and the risk of death. In fact, lithium can also be studied for earlier use, such as at the time of diagnosis, in order to avoid hospitalization altogether, as well as in the treatment of “Long Covid” syndromes. From the “Big Bang” to its presence in all living things, to its use in medicine, and in the storage of electricity, the third element of the Periodic Table may be paramount in life, which cannot be spelled without Li.
This clinical trial demonstrates that lithium deserves to be investigated in-depth and with a larger number of patients to treat COVID-19 in severe patients.
Data Availability Statement
The raw data supporting the conclusions of this article will be made available by the authors, without undue reservation.
Ethics Statement
The studies involving human participants were reviewed and approved by Ethics Committee of the Galician Network of Research Ethics Committees (protocol code 2020/238, approval date 30/09/2020) and approval of the clinical trial by the AEMPS 06/06/2020 with number EudraCT 2020–002008–37. The patients/participants provided their written informed consent to participate in this study.
Author Contributions
CS, TR-B, ML-G, DR-A, and JMO designed the study and contributed to data analysis/interpretation, ML-G, TÁ-E, AM, MI-M-A, LF-M, MP-R, AP-G, AL-D, ML-S, AS-D, AA-A, DM-R, and JMO performed the patient recruitment and treatments, SG, CS, and JMO contributed to data analysis/interpretation, MC, DV-F, BR, and JMO designed the study, and CS and JMO wrote the manuscript. All authors approved the final manuscript.
Funding
This research was funded by FCT, Fundação para a Ciência e Tecnologia, grant number SFRH/BD/135623/2018 and GAIN grant number IN607B2021/12 and IN606A-2019/022; and donations received by unknow individuals and from Mental Health Service of SERGAS and Hospital management from Hospital Álvaro Cunqueiro. Instituto de Salud Carlos III grant number CM20/00,243.
Conflict of Interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Publisher’s Note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
Acknowledgments
The authors would like to thank the Galicia Sur Health Research Institute (Instituto de Investigación Sanitaria Galicia Sur), the University Hospital Complex of Vigo (Complexo Hospitalario Universitario de Vigo), Hospital management, and María Tajes, head of the Mental Health Service of SERGAS for their support. In addition, the authors are especially thankful for the aid provided by the Internal Medicine Nursing staff, personnel from Internal Care Unit and technicians from Microbiology Service of the Álvaro Cunqueiro Hospital. We want to particularly acknowledge the patients and the Biobank at the Galicia Sur Health Research Institute for their collaboration. The authors would like to express their special thanks to Pablo Fuente for his help in the communication and dissemination of this work, as well as for the donations received from anonymous individuals.
Supplementary Material
The Supplementary Material for this article can be found online at: https://www.frontiersin.org/articles/10.3389/fphar.2022.850583/full#supplementary-material
References
Amsterdam, J. D., Maislin, G., and Rybakowski, J. (1990). A Possible Antiviral Action of Lithium Carbonate in Herpes Simplex Virus Infections. Biol. Psychiatry 27, 447–453. doi:10.1016/0006-3223(90)90555-G
PubMed Abstract | CrossRef Full Text | Google Scholar
Andrews, D. M., Estcourt, M. J., Andoniou, C. E., Wikstrom, M. E., Khong, A., Voigt, V., et al. (2010). Innate Immunity Defines the Capacity of Antiviral T Cells to Limit Persistent Infection. J. Exp. Med. 207, 1333–1343. doi:10.1084/JEM.20091193
PubMed Abstract | CrossRef Full Text | Google Scholar
Antia, R., Regoes, R. R., Koella, J. C., and Bergstrom, C. T. (2003). The Role of Evolution in the Emergence of Infectious Diseases. Nature 426, 658–661. doi:10.1038/nature02104
PubMed Abstract | CrossRef Full Text | Google Scholar
Ayuso, J. L. (1994). Use of Psychotropic Drugs in Patients with HIV Infection. Drugs 47, 599–610. doi:10.2165/00003495-199447040-00004
PubMed Abstract | CrossRef Full Text | Google Scholar
Barr, R. D., and Galbraith, P. R. (1983). Lithium and Hematopoiesis. Can. Med. Assoc. J. 128, 123–126. doi:10.1016/0370-2693(83)90925-5
PubMed Abstract | CrossRef Full Text | Google Scholar
Bschor, T. (1999). Complete Suppression of Recurrent Herpes Labialis with Lithium Carbonate. Pharmacopsychiatry 32, 158. doi:10.1055/s-2007-979224
PubMed Abstract | CrossRef Full Text | Google Scholar
Cascella, M., Rajnik, M., Aleem, A., Dulebohn, S. C., and Di Napoli, R. (2022). “Features, Evaluation and Treatment Coronavirus (COVID-19),” in StatPearls [Internet] (Treasure Island, FL: StatPearls Publishing).
Castillo-Quan, J. I., Li, L., Kinghorn, K. J., Ivanov, D. K., Tain, L. S., Slack, C., et al. (2016). Lithium Promotes Longevity through GSK3/NRF2-dependent Hormesis. Cell Rep 15, 638–650. doi:10.1016/j.celrep.2016.03.041
PubMed Abstract | CrossRef Full Text | Google Scholar
Chen, Z. Y., Raghav, K., Lieu, C. H., Jiang, Z. Q., Eng, C., Vauthey, J. N., et al. (2015). Cytokine Profile and Prognostic Significance of High Neutrophil-Lymphocyte Ratio in Colorectal Cancer. Br. J. Cancer 112, 1088–1097. doi:10.1038/bjc.2015.61
PubMed Abstract | CrossRef Full Text | Google Scholar
Costela-Ruiz, V. J., Illescas-Montes, R., Puerta-Puerta, J. M., Ruiz, C., and Melguizo-Rodríguez, L. (2020). SARS-CoV-2 Infection: The Role of Cytokines in COVID-19 Disease. Cytokine Growth Factor. Rev. 54, 62–75. doi:10.1016/J.CYTOGFR.2020.06.001
PubMed Abstract | CrossRef Full Text | Google Scholar
Cui, J., Xie, J., Gao, M., Zhou, H., Chen, Y., Cui, T., et al. (2015). Inhibitory Effects of Lithium Chloride on Replication of Type II Porcine Reproductive and Respiratory Syndrome Virus In Vitro. Antivir. Ther. 20, 565–572. doi:10.3851/IMP2924
PubMed Abstract | CrossRef Full Text | Google Scholar
Cunningham, A. C., Goh, H. P., and Koh, D. (2020). Treatment of COVID-19: Old Tricks for New Challenges. Crit. Care 24, 91–92. doi:10.1186/s13054-020-2818-6
PubMed Abstract | CrossRef Full Text | Google Scholar
De Clercq, E., and Li, G. (2016). Approved Antiviral Drugs over the Past 50 Years. Clin. Microbiol. Rev. 29, 695–747. doi:10.1128/CMR.00102-15
PubMed Abstract | CrossRef Full Text | Google Scholar
Duvall, A., and Gallicchio, V. S. (2017). Lithium Treatment in Clinical Medicine: History, Current Status and Future Use. J. Cell Sci. Ther. 8, 270. doi:10.4172/2157-7013
CrossRef Full Text | Google Scholar
Ekşioğlu‐Demiralp, E., Alan, S., Sili, U., Bakan, D., Ocak, İ., Yürekli, R., et al. (2021). Peripheral Innate and Adaptive Immune Cells during COVID ‐19: Functional Neutrophils, Pro‐inflammatory Monocytes, and Half‐dead Lymphocytes. Cytometry B Clin. 102, 153–167. doi:10.1002/CYTO.B.22042
CrossRef Full Text | Google Scholar
Everall, I. P., Bell, C., Mallory, M., Langford, D., Adame, A., Rockestein, E., et al. (2002). Lithium Ameliorates HIV-Gp120-Mediated Neurotoxicity. Mol. Cell. Neurosci. 21, 493–501. doi:10.1006/MCNE.2002.1196
PubMed Abstract | CrossRef Full Text | Google Scholar
Fathi, N., and Rezaei, N. (2020). Lymphopenia in COVID-19: Therapeutic Opportunities. Cell Biol. Int. 44, 1792–1797. doi:10.1002/CBIN.11403
PubMed Abstract | CrossRef Full Text | Google Scholar
Gallicchio, V. S., and Chen, M. G. (1981). Influence of Lithium on Proliferation of Hematopoietic Stem Cells. Exp. Hematol. 9, 804–810.
PubMed Abstract | Google Scholar
Gallicchio, V. S., Cibull, M. L., Hughes, N. K., and Tse, K.-F. (1993). Effect of Lithium in Murine Immunodeficiency Virus Infected Animals. Pathobiology 61, 216–221. doi:10.1159/000163797
PubMed Abstract | CrossRef Full Text | Google Scholar
Gao, J., Tian, Z., and Yang, X. (2020). Breakthrough: Chloroquine Phosphate Has Shown Apparent Efficacy in Treatment of COVID-19 Associated Pneumonia in Clinical Studies. Biosci. Trends 14, 72–73. doi:10.5582/bst.2020.01047
PubMed Abstract | CrossRef Full Text | Google Scholar
Gómez-Bernal, G. (2020). Lithium for the 2019 Novel Coronavirus. Med. Hypotheses 142. doi:10.1016/j.mehy.2020.109822
CrossRef Full Text | Google Scholar
Greenwood, B. (2014). The Contribution of Vaccination to Global Health: Past, Present and Future. Philos. Trans. R. Soc. B Biol. Sci. 369, 1–9. doi:10.1098/rstb.2013.0433
CrossRef Full Text | Google Scholar
Gupta, A., Gonzalez-Rojas, Y., Juarez, E., Crespo Casal, M., Moya, J., Falci, D. R., et al. (2021). Early Treatment for Covid-19 with SARS-CoV-2 Neutralizing Antibody Sotrovimab. N. Engl. J. Med. 385, 1941–1950. doi:10.1056/NEJMOA2107934
PubMed Abstract | CrossRef Full Text | Google Scholar
Hao, H. P., Wen, L. B., Li, J., Wang, Y., Ni, B., Wang, R., et al. (2015). LiCl Inhibits PRRSV Infection by Enhancing Wnt/β-Catenin Pathway and Suppressing Inflammatory Responses. Antivir. Res 117, 99–109. doi:10.1016/j.antiviral.2015.02.010
PubMed Abstract | CrossRef Full Text | Google Scholar
Harrison, S. M., Tarpey, I., Rothwell, L., Kaiser, P., and Hiscox, J. A. (2007). Lithium Chloride Inhibits the Coronavirus Infectious Bronchitis Virus in Cell Culture. Avian Pathol. 36, 109–114. doi:10.1080/03079450601156083
PubMed Abstract | CrossRef Full Text | Google Scholar
Hashimoto, S., Yoshizaki, K., Uno, K., Kitajima, H., Arai, T., Tamura, Y., et al. (2021). Prompt Reduction in CRP, IL-6, IFN-γ, IP-10, and MCP-1 and a Relatively Low Basal Ratio of Ferritin/CRP Is Possibly Associated with the Efficacy of Tocilizumab Monotherapy in Severely to Critically Ill Patients with COVID-19. Front. Med. 8. doi:10.3389/FMED.2021.734838
CrossRef Full Text | Google Scholar
Hj, L., Ds, G., Yt, L., Ys, W., Hy, L., and J, Z. (2018). Antiviral Effect of Lithium Chloride on Porcine Epidemic Diarrhea Virus In Vitro. Res. Vet. Sci. 118, 288–294. doi:10.1016/J.RVSC.2018.03.002
PubMed Abstract | CrossRef Full Text | Google Scholar
Holman, W., Holman, W., McIntosh, S., Painter, W., Painter, G., Bush, J., et al. (2021). Accelerated First-In-Human Clinical Trial of EIDD-2801/MK-4482 (Molnupiravir), a Ribonucleoside Analog with Potent Antiviral Activity against SARS-CoV-2. Trials 22, 561. doi:10.1186/S13063-021-05538-5
PubMed Abstract | CrossRef Full Text | Google Scholar
Horby, P., Lim, W. S., Emberson, J. R., Mafham, M., Bell, J. L., Linsell, L., et al. (2021). Dexamethasone in Hospitalized Patients with Covid-19. N. Engl. J. Med. 384, 693–704. doi:10.1056/NEJMOA2021436
PubMed Abstract | CrossRef Full Text | Google Scholar
Ibáñez, F. J., Farías, M. A., Gonzalez-Troncoso, M. P., Corrales, N., Duarte, L. F., Retamal-Díaz, D., et al. (2018). Experimental Dissection of the Lytic Replication Cycles of Herpes Simplex Viruses In Vitro. Front. Microbiol. 9. doi:10.3389/FMICB.2018.02406
CrossRef Full Text | Google Scholar
Ja, Q., Td, G., and Hk, M. (2004). Molecular Effects of Lithium. Mol. Interv. 4, 259–272. doi:10.1124/MI.4.5.6
PubMed Abstract | CrossRef Full Text | Google Scholar
Karampitsakos, T., Malakounidou, E., Papaioannou, O., Dimakopoulou, V., Zarkadi, E., Katsaras, M., et al. (2021). Tocilizumab Improves 28-day Survival in Hospitalized Patients with Severe COVID-19: an Open Label, Prospective Study. Respir. Res. 22, 317. doi:10.1186/S12931-021-01914-6
PubMed Abstract | CrossRef Full Text | Google Scholar
Kaushal, K., Kaur, H., Sarma, P., Bhattacharyya, A., Sharma, D. J., Prajapat, M., et al. (2021). Serum Ferritin as a Predictive Biomarker in COVID-19. A Systematic Review, Meta-Analysis and Meta-Regression Analysis. J. Crit. Care 67, 172–181. doi:10.1016/J.JCRC.2021.09.023
PubMed Abstract | CrossRef Full Text | Google Scholar
Kesmez Can, F., Özkurt, Z., Öztürk, N., and Sezen, S. (2021). Effect of IL-6, IL-8/CXCL8, IP-10/CXCL 10 Levels on the Severity in COVID 19 Infection. Int. J. Clin. Pract. 75 (12), e14970. doi:10.1111/IJCP.14970
PubMed Abstract | CrossRef Full Text | Google Scholar
Khosravi, M. (2021). Candidate Psychotropics against SARS – CoV – 2: A Narrative Review. Pharmacopsychiatry 55 (1), 16–23. doi:10.1055/A-1551-3756
PubMed Abstract | CrossRef Full Text | Google Scholar
Kibirige, D., Luzinda, K., and Ssekitoleko, R. (2013). Spectrum of Lithium Induced Thyroid Abnormalities: A Current Perspective. Thyroid Res. 6. doi:10.1186/1756-6614-6-3
PubMed Abstract | CrossRef Full Text | Google Scholar
Lauer, S. A., Grantz, K. H., Bi, Q., Jones, F. K., Zheng, Q., Meredith, H. R., et al. (2020). The Incubation Period of Coronavirus Disease 2019 (COVID-19) from Publicly Reported Confirmed Cases: Estimation and Application. Ann. Intern. Med. 172, 577–582. doi:10.7326/M20-0504
PubMed Abstract | CrossRef Full Text | Google Scholar
Li, H. J., Gao, D. S., Li, Y. T., Wang, Y. S., Liu, H. Y., and Zhao, J. (2018). Antiviral Effect of Lithium Chloride on Porcine Epidemic Diarrhea Virus In Vitro. Res. Vet. Sci. 118, 288–294. doi:10.1016/j.rvsc.2018.03.002
PubMed Abstract | CrossRef Full Text | Google Scholar
Lucas, C., Wong, P., Klein, J., Castro, T. B. R., Silva, J., Sundaram, M., et al. (2020). Longitudinal Analyses Reveal Immunological Misfiring in Severe COVID-19. Nature 584, 463–469. doi:10.1038/S41586-020-2588-Y
PubMed Abstract | CrossRef Full Text | Google Scholar
Mahase, E. (2021). Covid-19: Pfizer’s Paxlovid Is 89% Effective in Patients at Risk of Serious Illness, Company Reports. BMJ 375, n2713. doi:10.1136/BMJ.N2713
PubMed Abstract | CrossRef Full Text | Google Scholar
Makola, R. T., Kgaladi, J., More, G. K., Jansen van Vuren, P., Paweska, J. T., and Matsebatlela, T. M. (2021). Lithium Inhibits NF-Κb Nuclear Translocation and Modulate Inflammation Profiles in Rift valley Fever Virus-Infected Raw 264.7 Macrophages. Virol. J. 18. doi:10.1186/S12985-021-01579-Z
PubMed Abstract | CrossRef Full Text | Google Scholar
Mariette, X., Hermine, O., Tharaux, P.-L., Resche-Rigon, M., Porcher, R., Ravaud, P., et al. (2022). Sarilumab in Adults Hospitalised with Moderate-To-Severe COVID-19 Pneumonia (CORIMUNO-SARI-1): An Open-Label Randomised Controlled Trial. Lancet Rheumatol. 4. doi:10.1016/S2665-9913(21)00315-5
CrossRef Full Text | Google Scholar
Munch, M. W., Myatra, S. N., Vijayaraghavan, B. K. T., Saseedharan, S., Benfield, T., Wahlin, R. R., et al. (2021). Effect of 12 Mg vs 6 Mg of Dexamethasone on the Number of Days Alive without Life Support in Adults with COVID-19 and Severe Hypoxemia: The COVID STEROID 2 Randomized Trial. JAMA 326, 1807–1817. doi:10.1001/JAMA.2021.18295
PubMed Abstract | CrossRef Full Text | Google Scholar
Murru, A., Manchia, M., Hajek, T., Nielsen, R. E., Rybakowski, J. K., Sani, G., et al. (2020). Lithium’s Antiviral Effects: a Potential Drug for CoViD-19 Disease? Int. J. Bipolar Disord. 8. doi:10.1186/S40345-020-00191-4
PubMed Abstract | CrossRef Full Text | Google Scholar
Oldstone, M. B., Tishon, A., Eddleston, M., de la Torre, J. C., McKee, T., and Whitton, J. L. (1993). Vaccination to Prevent Persistent Viral Infection. J. Virol. 67, 4372–4378. doi:10.1128/jvi.67.7.4372-4378.1993
PubMed Abstract | CrossRef Full Text | Google Scholar
Pietruczuk, K., Lisowska, K. A., Grabowski, K., Landowski, J., and Witkowski, J. M. (2018). Proliferation and Apoptosis of T Lymphocytes in Patients with Bipolar Disorder. Sci. Rep. 8. doi:10.1038/s41598-018-21769-0
PubMed Abstract | CrossRef Full Text | Google Scholar
Puertas, M. C., Salgado, M., Morón-López, S., Ouchi, D., Muñoz-Moreno, J. A., Moltó, J., et al. (2014). Effect of Lithium on HIV-1 Expression and Proviral Reservoir Size in the CD4+ T Cells of Antiretroviral Therapy Suppressed Patients. AIDS 28, 2157–2159. doi:10.1097/QAD.0000000000000374
PubMed Abstract | CrossRef Full Text | Google Scholar
Qin, C., Zhou, L., Hu, Z., Zhang, S., Yang, S., Tao, Y., et al. (2020). Dysregulation of Immune Response in Patients with Coronavirus 2019 (COVID-19) in Wuhan, China. Clin. Infect. Dis. 71, 762–768. doi:10.1093/CID/CIAA248
PubMed Abstract | CrossRef Full Text | Google Scholar
Quiroz, J. A., Machado-Vieira, R., Zarate, C. A., and Manji, H. K. (2010). Novel Insights into Lithium’s Mechanism of Action: Neurotrophic and Neuroprotective Effects. Neuropsychobiology 62, 50–60. doi:10.1159/000314310
PubMed Abstract | CrossRef Full Text | Google Scholar
Rosen, M. S. (2017). Lithium in Child and Adolescent Bipolar Disorder. Am. J. Psychiatry Resid. J. 12, 3–5. doi:10.1176/appi.ajp-rj.2017.120202
CrossRef Full Text | Google Scholar
Rostami, M., and Mansouritorghabeh, H. (2020). D-dimer Level in COVID-19 Infection: a Systematic Review. Expert Rev. Hematol. 13, 1265–1275. doi:10.1080/17474086.2020.1831383
PubMed Abstract | CrossRef Full Text | Google Scholar
Rudd, C. E. (2020). GSK-3 Inhibition as a Therapeutic Approach against SARs CoV2: Dual Benefit of Inhibiting Viral Replication while Potentiating the Immune Response. Front. Immunol. 11. doi:10.3389/fimmu.2020.01638
PubMed Abstract | CrossRef Full Text | Google Scholar
Sabbatino, F., Conti, V., Franci, G., Sellitto, C., Manzo, V., Pagliano, P., et al. (2021). PD-L1 Dysregulation in COVID-19 Patients. Front. Immunol. 12. doi:10.3389/FIMMU.2021.695242
CrossRef Full Text | Google Scholar
Shorter, E. (2009). The History of Lithium Therapy. Bipolar Disord. 11, 4–9. doi:10.1111/j.1399-5618.2009.00706.x
PubMed Abstract | CrossRef Full Text | Google Scholar
Skinner, G. R. B., Hartley, C., Buchan, A., Harper, L., and Gallimore, P. (1980). The Effect of Lithium Chloride on the Replication of Herpes Simplex Virus. Med. Microbiol. Immunol. 168, 139–148. doi:10.1007/BF02121762
PubMed Abstract | CrossRef Full Text | Google Scholar
Spuch, C., López-García, M., Rivera-Baltanás, T., Rodrígues-Amorím, D., and Olivares, J. M. (2020). Does Lithium Deserve a Place in the Treatment against COVID-19? A Preliminary Observational Study in Six Patients, Case Report. Front. Pharmacol. 11. doi:10.3389/fphar.2020.557629
PubMed Abstract | CrossRef Full Text | Google Scholar
Sui, X., Yin, J., and Ren, X. (2010). Antiviral Effect of Diammonium Glycyrrhizinate and Lithium Chloride on Cell Infection by Pseudorabies Herpesvirus. Antivir. Res 85, 346–353. doi:10.1016/j.antiviral.2009.10.014
PubMed Abstract | CrossRef Full Text | Google Scholar
Tan, C., Huang, Y., Shi, F., Tan, K., Ma, Q., Chen, Y., et al. (2020a). C-reactive Protein Correlates with CT Findings and Predicts Severe COVID-19 Early. J. Med. Virol. 92 (7), 856–862. doi:10.1002/jmv.25871
PubMed Abstract | CrossRef Full Text | Google Scholar
Tan, L., Wang, Q., Zhang, D., Ding, J., Huang, Q., Tang, Y. Q., et al. (2020b). Lymphopenia Predicts Disease Severity of COVID-19: a Descriptive and Predictive Study. Signal. Transduct. Target. Ther. 5. doi:10.1038/S41392-020-0148-4
PubMed Abstract | CrossRef Full Text | Google Scholar
Tavakolpour, S., Rakhshandehroo, T., Wei, E. X., and Rashidian, M. (2020). Lymphopenia during the COVID-19 Infection: What it Shows and what Can Be Learned. Immunol. Lett. 225, 31–32. doi:10.1016/J.IMLET.2020.06.013
PubMed Abstract | CrossRef Full Text | Google Scholar
Terpos, E., Ntanasis-Stathopoulos, I., Elalamy, I., Kastritis, E., Sergentanis, T. N., Politou, M., et al. (2020). Hematological Findings and Complications of COVID-19. Am. J. Hematol. 95, 834–847. doi:10.1002/ajh.25829
PubMed Abstract | CrossRef Full Text | Google Scholar
Ueland, T., Heggelund, L., Lind, A., Holten, A. R., Tonby, K., Michelsen, A. E., et al. (2021). Elevated Plasma sTIM-3 Levels in Patients with Severe COVID-19. J. Allergy Clin. Immunol. 147, 92–98. doi:10.1016/J.JACI.2020.09.007
PubMed Abstract | CrossRef Full Text | Google Scholar
Wang, Y., Zhang, D., Du, G., Du, R., Zhao, J., Jin, Y., et al. (2020). Remdesivir in Adults with Severe COVID-19: a Randomised, Double-Blind, Placebo-Controlled, Multicentre Trial. Lancet (London, England) 395, 1569–1578. doi:10.1016/S0140-6736(20)31022-9
PubMed Abstract | CrossRef Full Text | Google Scholar
Willyard, C. (2021). How Antiviral Pill Molnupiravir Shot Ahead in the COVID Drug hunt. Nature 1, 1. doi:10.1038/D41586-021-02783-1
CrossRef Full Text | Google Scholar
Won, E., and Kim, Y. K. (2017). An Oldie but Goodie: Lithium in the Treatment of Bipolar Disorder through Neuroprotective and Neurotrophic Mechanisms. Int. J. Mol. Sci. 18. doi:10.3390/ijms18122679
PubMed Abstract | CrossRef Full Text | Google Scholar
Wong, R. S. Y. (2020). The SARS-CoV-2 Outbreak: an Epidemiological and Clinical Perspective. SN Compr. Clin. Med. 2, 1983–1991. doi:10.1007/S42399-020-00546-Z
PubMed Abstract | CrossRef Full Text | Google Scholar
Woolhouse, M., Scott, F., Hudson, Z., Howey, R., and Chase-Topping, M. (2012). Human Viruses: Discovery and Emeraence. Philos. Trans. R. Soc. B Biol. Sci. 367, 2864–2871. doi:10.1098/rstb.2011.0354
PubMed Abstract | CrossRef Full Text | Google Scholar
Yamauchi, Y., and Helenius, A. (2013). Virus Entry at a Glance. J. Cell Sci. 126, 1289–1295. doi:10.1242/jcs.119685
PubMed Abstract | CrossRef Full Text | Google Scholar
Zhao, Y., Yan, K., Wang, Y., Cai, J., Wei, L., Li, S., et al. (2020). Lithium Chloride Confers protection against Viral Myocarditis via Suppression of Coxsackievirus B3 Virus Replication. Microb. Pathog. 144, 104169. doi:10.1016/j.micpath.2020.104169
PubMed Abstract | CrossRef Full Text | Google Scholar
Zhou, P., Fu, X., Yan, Z., Fang, B., Huang, S., Fu, C., et al. (2015). Antiviral Effect of Lithium Chloride on Infection of Cells by Canine Parvovirus. Arch. Virol. 160, 2799–2805. doi:10.1007/s00705-015-2577-x
PubMed Abstract | CrossRef Full Text | Google Scholar
Ziaie, Z., and Kefalides, N. A. (1989). Lithium Chloride Restores Host Protein Synthesis in Herpes Simplex Virus-Infected Endothelial Cells. Biochem. Biophys. Res. Commun. 160, 1073–1078. doi:10.1016/S0006-291X(89)80112-3
Browse Studies
Should We All Take a Bit of Lithium?
The idea of putting a mind-altering drug in the drinking water is the stuff of sci-fi, terrorist plots and totalitarian governments. Considering the outcry that occurred when putting fluoride in the water was first proposed, one can only imagine the furor that would...
Lithium treatment and human hippocampal neurogenesis
There is a PDF available for this article. Please click here to read the article.Source: https://www.nature.com/articles/s41398-021-01695-yBrowse Studies
A Low Dose of Lithium May Slow Kidney Aging
Best known therapeutically as a treatment for bipolar disorder, lithium has long intrigued researchers with its potential age-defying properties. The element has been shown in lab experiments to extend the lifespan of fruit flies and roundworms, while observational...
Beyond its psychiatric use: the benefits of low dose lithium supplementation
Sophie I Hamstra 1, Brian D Roy 1, Peter Tiidus 1, Adam J MacNeil 2, Panagiota Klentrou 1, Rebecca E K MacPherson 2, Val A Fajardo 1 Affiliations 1Department of Kinesiology, Brock University, St. Catharines, ON. 2Department of Health Sciences, Brock University, St....
Systems Biology Understanding of the Effects of Lithium on Cancer
Weihao Ge1,2 Eric Jakobsson1,2,3* 1National Center for Supercomputing Applications, University of Illinois at Urbana-Champaign, Urbana, IL, United States 2Center for Biophysics and Computational Biology, University of Illinois at Urbana-Champaign, Urbana, IL, United...
Low-dose lithium impact in an addiction treatment setting
There is a PDF available for this article. Please click here to read the article. Source: https://www.sciencedirect.com/science/article/pii/S2468171720300053 Browse Studies
Lithium in Drinking Water and the Incidences of Crimes, Suicides, and Arrests Related to Drug Addictions
G N Schrauzer 1, K P Shrestha PMID: 1699579 DOI: 10.1007/BF02990271 Abstract Using data for 27 Texas counties from 1978-1987, it is shown that the incidence rates of suicide, homicide, and rape are significantly higher in counties whose drinking water supplies contain...